


Introduction
When did your monitoring team last anticipate and prevent a protocol deviation?
This question goes to the core of ICH E6(R3), which brings the biggest update to Good Clinical Practice (GCP) standards in almost ten years. On January 6, 2025, the International Council for Harmonisation (ICH) adopted E6(R3) Principles and Annex 1. This marks a major change from checking compliance after the fact to managing quality from the beginning.
The timeline is tight. The TGA is publishing Australian-specific annotations through Q3 2025, with full implementation projected for Q1 2026. More urgently, the European Medicines Agency has announced an effective date of July 23, 2025. If you’re running trials with EU sites, your compliance deadline is not 2026. It has already passed.
This guide explains the core changes in E6(R3), what they mean for Australian sponsors in practical terms, and provides implementation frameworks you can apply immediately.
The Regulatory Context
ICH E6 evolved from foundational GCP (E6[R1]), to risk-based but procedural guidance (E6[R2]), to the principle- and annex-driven E6(R3) restructuring.
E6(R3) now includes a Principles document and annexes: Annex 1 covers conventional trials; Annex 2 (in progress) will address decentralized approaches.
The rise of decentralized trials, wearables, and remote monitoring—mainstream post-COVID—demanded specific E6(R3) guidance.
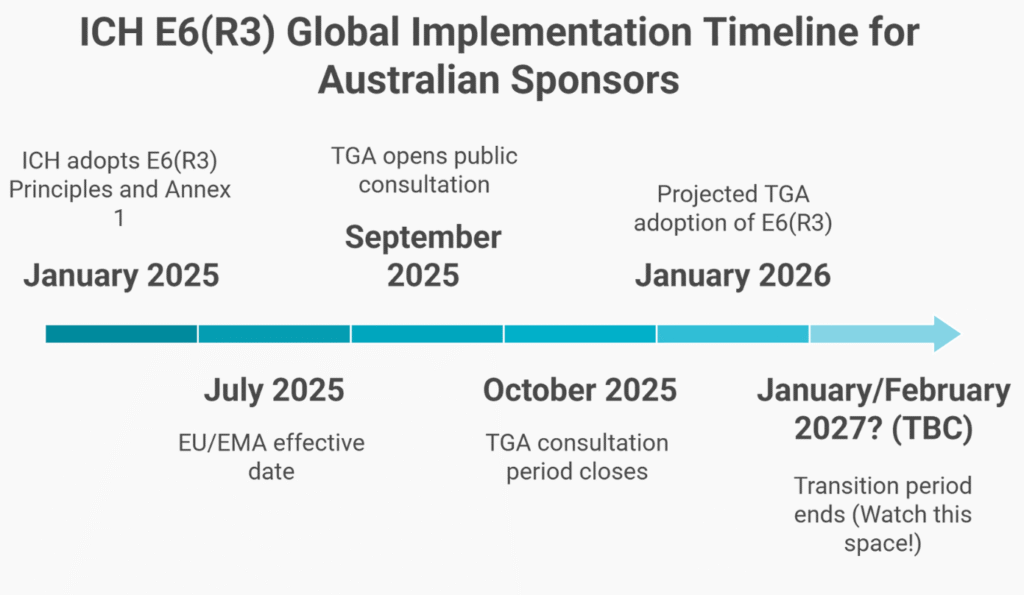
Timeline
- January 6, 2025: ICH adoption (Step 4)
- July 23, 2025: EMA/EU implementation (effective immediately)
- TGA will release annotations by Q3 2025; implementation is projected for early 2026.
This staggered timeline means EU sites must comply by July 2025, while Australia has until early 2026—raising inspection risks if you use dual frameworks.
Practical Implications for Australian Sponsors
QMS Transformation Required
You cannot simply revise your monitoring SOP because E6(R3) requires a shift from procedure-based compliance to principle-based quality management.
E6(R2) thinking:
- The monitoring SOP defines the visit frequency and the SDV percentage.
- Quality metrics track procedure compliance
- Training emphasizes following SOPs.
E6(R3) thinking:
- The Risk-Based Quality Management Framework defines CtQ methodology.
- Quality tolerance limits define acceptable variation.
- Monitoring plans are trial-specific, derived from risk.
- Training emphasizes risk-based decision-making.
You need to rewrite your QMS, not just update your SOPs. Allow 3-6 months for framework development, process redesign, training, and system updates. Vendor Agreements Need Overhaul
Every Master Service Agreement requires revision for:
Data governance:
- Who validates systems
- Who verifies fitness-for-purpose
- Audit trail management
- System defect reporting
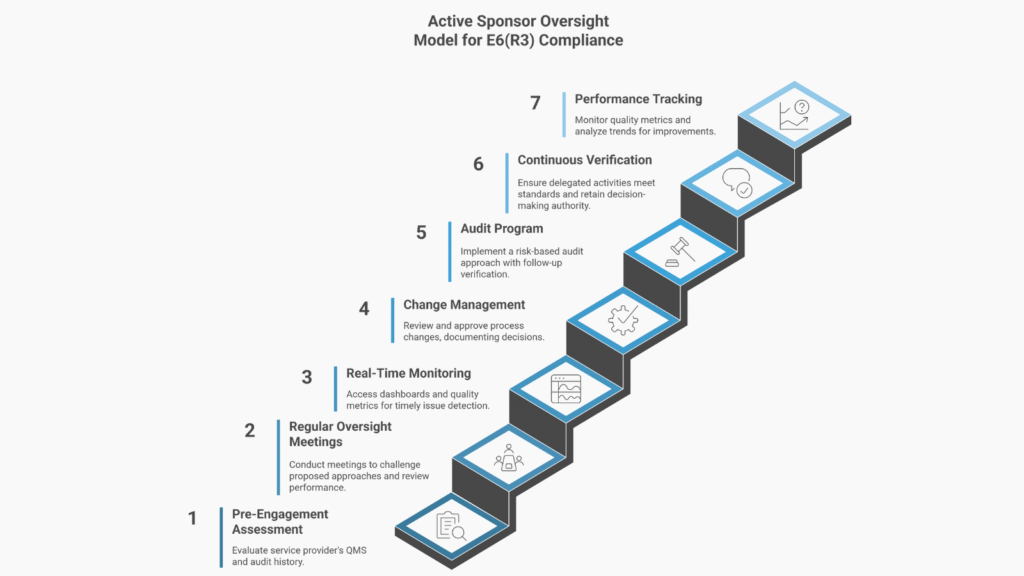
Active oversight:
- Meeting cadence and documentation
- Performance metrics and reporting frequency
- Sponsor system access
- Escalation triggers and timeframes
Quality alignment:
- The service provider approach must align with the sponsor’s risk assessment.
- CtQ factors drive service provider activities.
- Quality tolerance limits are contractually defined.
The Global Compliance Challenge: Australian sponsors running global trials face an urgent choice: harmonize frameworks or create critical inspection risk now. Waiting is not an option; dual systems invite immediate regulatory scrutiny.
A Phase III trial starting January 2026 with Melbourne and Munich sites faces:
- Australian sites: Could operate under E6(R2) during transition
- EU sites: Must comply with E6(R3) from July 2025. If you postpone implementing E6(R3) until required by the TGA, your EU sites are instantly non-compliant. EMA inspections will uncover inadequate quality management, which can immediately affect submission timelines. Delay directly threatens your global trial success.
Strategic response: Implement E6(R3)-compliant systems by Q2 2025 if operating globally.

