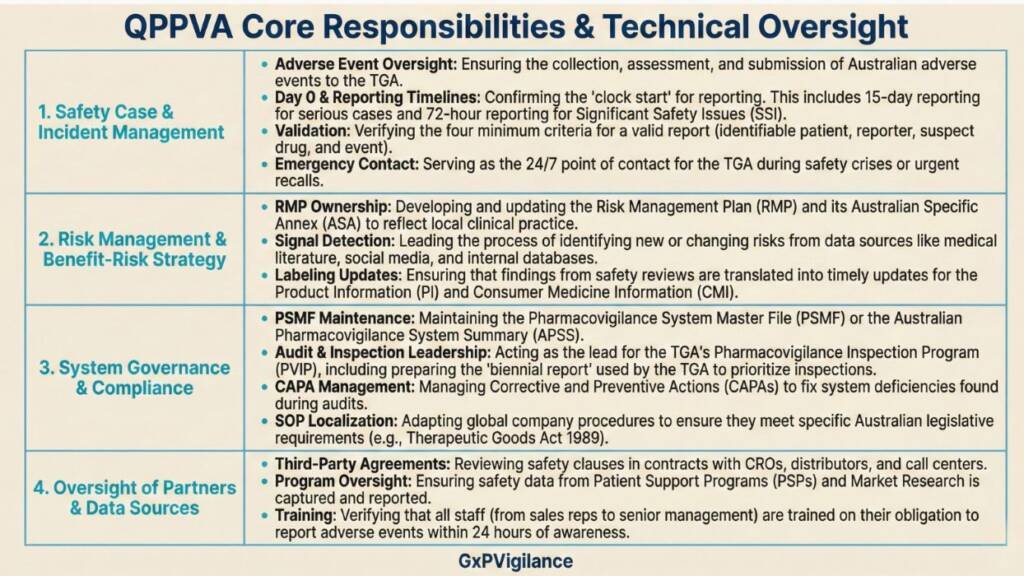
Core responsibilities include:
The “Fractional QPPV” Model: Many Australian biotechs and international sponsors use consultants as fractional QPPVs. A single consultant manages 3-10 clients, providing named oversight at a fraction of the cost of a full-time hire. This model reduces compliance costs by approximately 80% compared to traditional internal staffing while providing access to senior expertise. A pre-revenue biotech with one Phase II product faces the same regulatory obligations as a top-tier multinational; the fractional model makes this manageable.
How the Pharmacovigilance Consultant in Australia Is Adapting to AI
AI is not replacing consultants in Australia. It is shifting their value proposition from data processing to oversight and validation—a significant distinction that sponsors and practitioners need to understand clearly.
Example: Historically, 60-80% of a consultant’s billable time was spent on manual tasks: reading emails, entering data into safety databases, selecting MedDRA codes, and drafting case narratives. AI-enabled workflows now automate much of this work. Natural language processing extracts adverse event elements from unstructured sources—such as physician notes, call centre transcripts, and patient emails. Machine learning drafts case narratives and suggests coding. Literature surveillance tools triage thousands of abstracts in minutes, presenting only high-probability articles for human review.
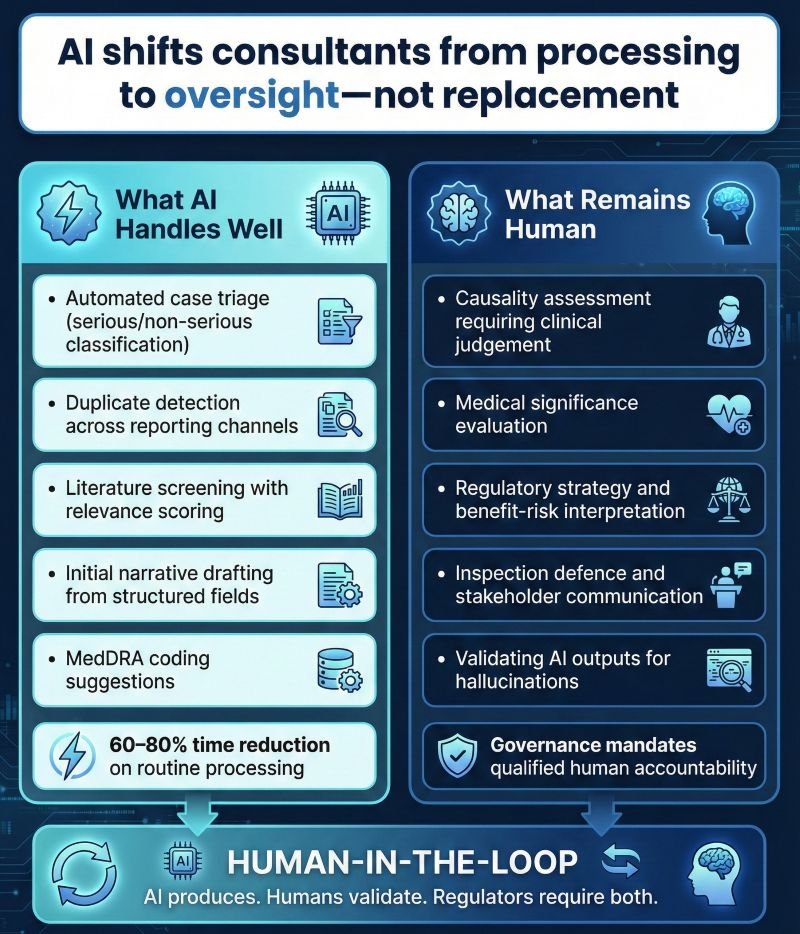
What AI handles well:
- Automated case triage (serious/non-serious, expected/unexpected classification)
- Duplicate detection across multiple reporting channels
- Literature screening with relevance scoring
- Initial narrative drafting from structured data fields
- MedDRA coding suggestions based on reporter descriptions
- Causality assessment requires clinical judgement
- Medical significance evaluation in ambiguous cases
- Regulatory strategy decisions and benefit-risk interpretation
- Inspection defence and stakeholder communication
- Validating AI outputs for accuracy and “hallucinations”
This creates the “Human-in-the-Loop” operational model now standard in compliant AI pharmacovigilance. The TGA and other global regulators mandate that a qualified human must retain ultimate responsibility for the safety system. The consultant’s role shifts from writing reports to auditing AI outputs, checking for hallucinations, and ensuring medical logic holds.
Consultants are becoming prompt engineers—encoding their expertise into workflow logic—and validators, proving AI tools are fit for purpose under TGA expectations. Under GAMP 5 principles, AI tools often require validation documentation demonstrating they produce reliable, reproducible outputs. This validation work is itself becoming a new service line.
Practical checklist for sponsors evaluating PV consultants in 2026:
Verify Australian residency (non-negotiable for A-PVCP designation)
- Confirm direct TGA inspection experience.
- Assess therapeutic area expertise relevant to your products.
- Review their approach to AI tool validation (GAMP 5 alignment)
- Understand their oversight model for AI-generated outputs.
- Clarify liability coverage and professional indemnity insurance.
- Check their continuous professional development (ARCS, ISoP membership)
Business Model Implications for Consultants
The shift presents a billing paradox. If AI reduces case processing time by 80%, the traditional hourly billing model collapses. Consultants are adapting by moving toward value-based retainers and subscription models—selling “compliance-as-a-service” rather than charging by the hour for data entry.
New service lines are emerging: AI tool validation, workflow design, and training sponsors’ internal teams to use AI tools compliantly. Consultants who can design AI-integrated safety systems, write validation documentation, and apply critical human judgment to automated outputs command premium positioning.

What This Means for You
If you are a sponsor engaging a pharmacovigilance consultant in Australia, focus on functional capability rather than title alone. The gap between a named contact and genuine QPPV expertise is where inspection findings occur. Ask how they approach AI validation, understand their oversight model for automated outputs, and verify they can demonstrate TGA inspection readiness.
If you are considering PV consulting as a career path, recognise that data entry skills are becoming commoditised. Differentiation lies in clinical judgement, regulatory expertise, AI fluency, and the ability to communicate complex safety information across diverse audiences.
If you are already practising, invest in validating AI tools, building competencies, and developing prompt engineering. The profession is migrating from “processing” to “oversight and design.” The consultants who thrive will be those who can architect AI-integrated systems while maintaining the human judgment that regulators—and patients—require. Patient safety remains the anchor. AI speeds up and standardises pharmacovigilance, but it does not replace the clinical reasoning that transforms data into protection.