


Quality Management Systems in Australian Clinical Trials: The Regulatory Framework
Sponsors conducting clinical trials in Australia operate within overlapping governing frameworks. Each framework reinforces quality management obligations:
ICH GCP E6(R3): Principle 6 requires sponsors to build quality into scientific and operational design. Similarly, Principle 7 expects a proportionate process. Additionally, Principle 10 clarifies that sponsors retain responsibility even when they delegate activities.
NHMRC National Statement: Establishes ethical standards requiring scientifically sound designs that protect participants.
TGA Clinical Trial Notification (CTN) and Clinical Trial Approval (CTA) Schemes: Allow trials to proceed after ethics approval and TGA notification, placing greater self-regulatory responsibility on sponsors.
Many sponsors misunderstand one point: delegation does not transfer responsibility. When a sponsor engages a CRO to manage monitoring or data management, the CRO executes the work, but accountability for quality and integrity remains with the sponsor. Regulators assess systems and evidence, not intentions. An inspector will ask: “How did you maintain oversight?” rather than “Did you trust your CRO?”

What Is a Quality Management System in Clinical Trials?
A QMS in the clinical trial context comprises the organised structure of policies, procedures, responsibilities, and processes that ensure consistent conduct and controlled documentation across the trial lifecycle. Importantly, quality management systems in Australian clinical trials serve purposes extending beyond compliance:
Consistent trial conduct across sites and personnel
Controlled documentation with clear version management
Systematic risk identification and mitigation
Evidence of ongoing improvement
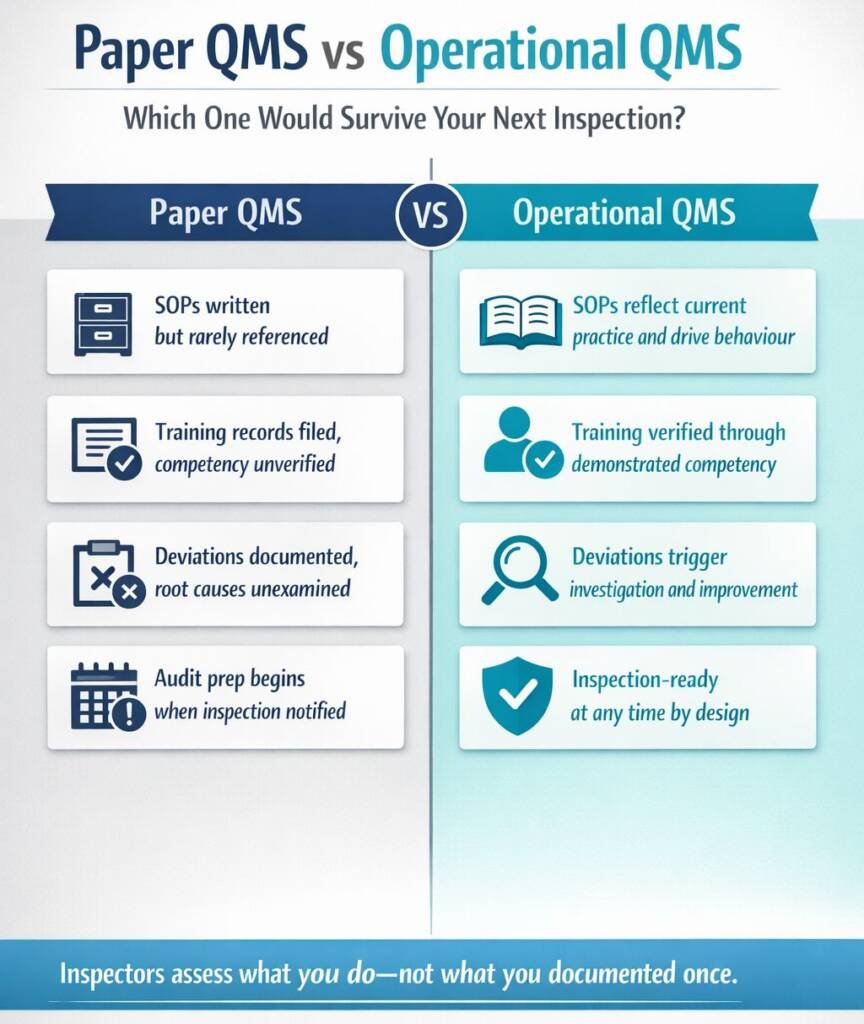
The distinction between a paper QMS and an operational QMS is important. A paper QMS exists in documented form, with SOPs written, training records filed, and processes described, but may not reflect how work actually gets done. An operational QMS is embedded in daily practice: staff follow procedures because they understand them, deviations trigger investigation, and feedback improves the system.
Sponsors should ask: “If an inspector walked through our operations today, might they see our documented system in action—or gaps between what we say and what we do?”
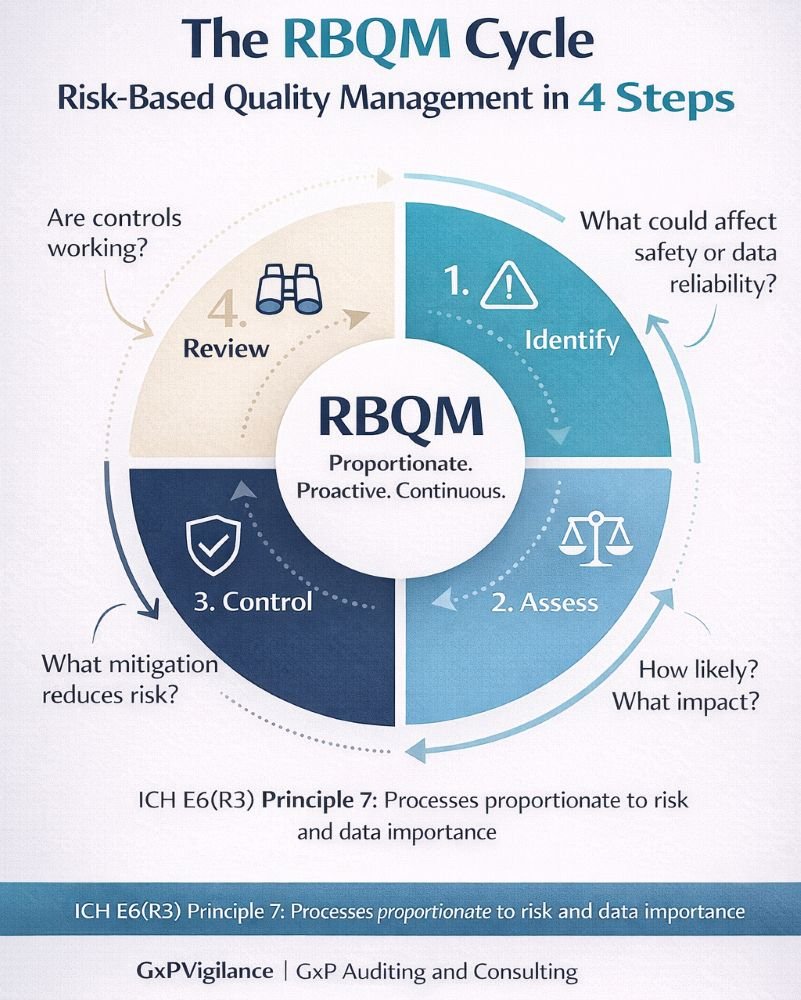
Risk-Based Quality Management in Practice
- Risk Identification: What could go wrong that affects participant safety or data reliability?
- Risk Assessment: How likely is each risk, and what is its potential impact?
- Risk Control: What mitigation strategies reduce the likelihood or impact?
- Risk Review: How do we monitor whether controls work effectively?
Sponsor Oversight: CROs, Vendors, and Delegated Activities
When sponsors delegate activities to CROs or vendors, they must maintain active oversight. This distinction is important during inspections.
Effective oversight mechanisms include:
- Metrics and KPIs tracking vendor performance against agreed standards
- Issue escalation pathways ensuring problems reach sponsor decision-makers
- Audit programs providing independent verification of vendor compliance
Regulators expect evidence of oversight, such as meeting minutes documenting performance reviews, correspondence addressing issues, and escalation records showing sponsor engagement. Sponsors who cannot provide this evidence will struggle to demonstrate oversight.
Aligning QMS With Inspection Readiness and Continuous Improvement
In Australian clinical trials, there is a key difference between inspection readiness and inspection panic. Inspection readiness means the QMS is up to date, staff follow processes, and evidence is always accessible. Inspection panic involves rushing to gather evidence after notification, exposing gaps between documented systems and actual practice.
Building inspection readiness requires:
- Regular internal audits identify issues before inspectors do
- Metrics review tracking QMS performance indicators
- CAPA effectiveness checks verifying that corrective actions achieve intended outcomes
- Feedback loops incorporating lessons learned into system improvements
A sustainable quality culture views audits as opportunities for improvement.
Conclusion: Quality Systems as a Sponsor’s Strategic Asset
- Risk protection, reducing regulatory findings, and trial disruption
- Trial enabler supporting efficient conduct through clear processes
- Confidence builder demonstrating to regulators, ethics committees, and partners that oversight is real
Sponsor accountability cannot be outsourced. Whether using an integrated corporate QMS or relying on CRO systems with hybrid oversight, sponsors must understand, implement, and defend their quality systems.
As ICH E6(R3) takes effect and TGA expectations evolve, the focus on proportionate, risk-based quality systems will increase. Sponsors who treat QMS as a strategic asset, rather than a compliance burden, will be better positioned to conduct trials that protect participants, generate reliable data, and withstand regulatory scrutiny.

