

Human-in-the-Loop AI in Pharma vs Human-on-the-Loop Oversight
Operational Risk Boundaries
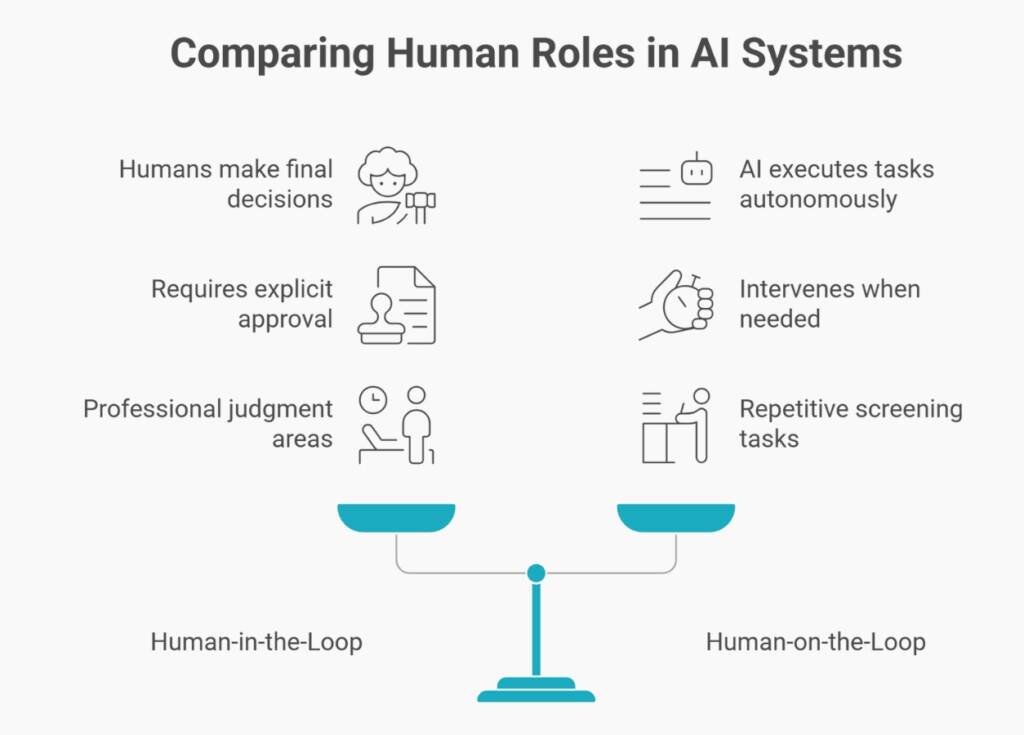
The distinction between HITL and HOTL defines where decision authority sits.
- Human-in-the-Loop (HITL) puts humans in the decision pathway: AI proposes, humans dispose. Every output requires explicit approval before it is entered into regulatory records. This applies where professional judgment is non-delegable, such as medical assessments, safety determinations, and regulatory strategy.
- Human-on-the-Loop (HOTL) positions humans as monitors. AI executes tasks within defined parameters. Humans watch performance and intervene when systems operate outside acceptable bounds. This suits repetitive screening—literature searches, formatting checks, completeness validations.
Regulatory teams must accurately classify each AI application. Using HOTL where HITL is required—allowing AI to auto-approve regulatory responses—creates accountability gaps that no retrospective review can close.
Operational vs. Performative HITL differentiates compliance from quality.
The Professional Liability Line
When companies outsource regulatory work to AI-using consultants, accountability becomes complex. The consultant generates content. The company reviews and submits. But if AI hallucinates data or mischaracterises safety findings, who bears liability?
Under GxP principles, both parties. Consultants deliver validated, accurate work. Companies verify accuracy before submission. HITL protects both by ensuring a qualified review at each handoff.
Recent legal precedents reinforce this—courts sanctioned professionals citing non-existent AI sources. In pharma, submitting unverified AI clinical data isn’t negligence—it’s potentially fraud. The Human-in-the-Loop serves as the insurer of reality.
What HITL Looks Like in Day-to-Day Regulatory Work
Document Drafting and Approval
When AI drafts regulatory content—Module 2.5 Clinical Overview, for example—the HITL workflow requires:
- System Action: AI generates a draft, logged with model version and timestamp
- Human Review: Writer validates factual claims against sources, checks citations, and adjusts language
- Documented Changes: Track-changes preserves AI output and human refinement separately
- Formal Approval: Qualified person applies an electronic signature, creating the required audit trail
The audit trail must distinguish AI contribution from human approval. Fifty pages of AI text approved with a single “I reviewed this” signature means HITL failed. Inspectors expect evidence of active validation—corrections made, sources verified, clinical judgment applied.
Pharmacovigilance Case Processing
AI screens adverse event databases, flags potential cases, and drafts narratives. The HITL requirement here is absolute. A QPPV or delegate must validate the four-element case definition, apply causality assessment using medical judgment (not AI inference), verify source accuracy, and determine reporting obligations.
AI accelerates screening—reducing 2,000 abstracts to 47 signals reviewed in 90 minutes instead of 8 hours. But causality remains human territory. If AI suggests causality based on statistical correlation without biological plausibility, and a human blindly approves it, the company triggers false signals with regulatory consequences.
Regulatory Intelligence
AI monitors authority websites, extracts guidance, and summarises changes. HITL converts this from a collection to a strategy. AI identifies the TGA updated device software guidance. Human-in-the-Loop contextualises: “This requires SaMD reclassification revalidation. Six weeks, $45,000. Recommend immediate action.”
AI provides information. Humans provide implication. Regulatory strategy demands an understanding of organisational priorities, risk tolerance, and the competitive context—where professional judgment remains essential.
When HITL Controls Break Down
HITL fails when approval is rubber-stamping (reviewers don’t read outputs), competency gaps exist (reviewers lack expertise), volume overwhelms capacity (too many outputs, too few reviewers), or audit trails are generic (logs show “approved” but not what was validated).
These failures convert HITL from control to theatre. When inspectors probe, organisations discover HITL was documented but not operationalised.
Consequence: regulatory findings citing inadequate oversight, submission delays pending validation evidence, and erosion of regulator confidence in quality systems.
Conclusion: The Regulatory Architect Role
Human-in-the-Loop AI in Pharma defines the future of pharmaceutical regulatory work. As AI capabilities expand, value shifts from content origination to validation expertise. The consultant who works AI-enabled but validation-assured delivers a sustainable advantage.
For Australian teams, proper HITL implementation means classifying AI by regulatory risk, defining approval authorities in SOPs, setting reviewer competency criteria, implementing audit trails separating AI from human actions, training for AI-specific validation, and adjusting workflows when quality drops.
Regulators won’t ask whether you used AI. They’ll ask whether you controlled it. Human-in-the-Loop is your answer—but only if implemented as the regulatory control it is, not the safety feature it’s marketed as.
AI accelerates drafting. Humans ensure accuracy. Audit trails prove accountability. Together, this is regulatory work fit for TGA scrutiny.

